Abstract
Background
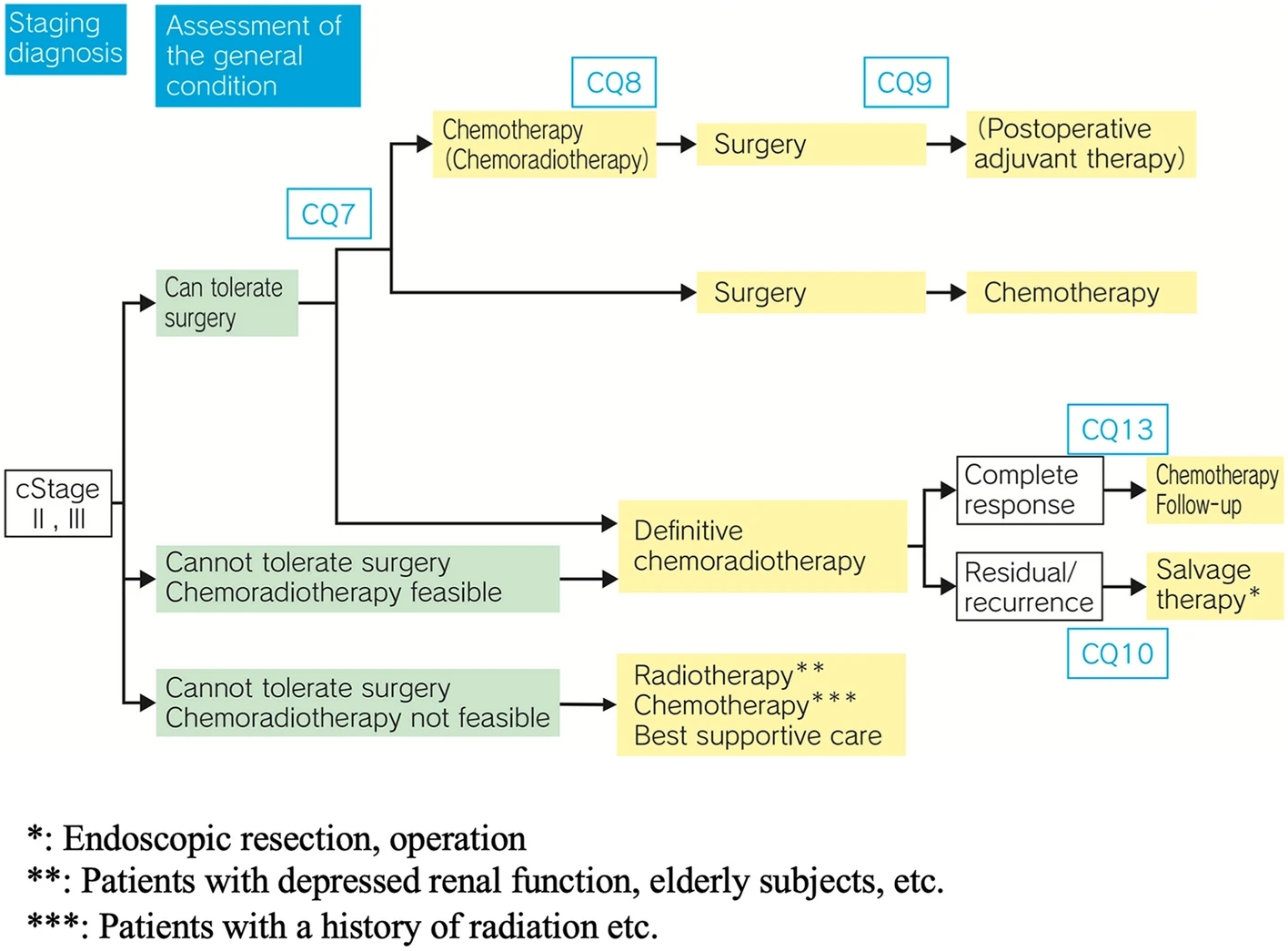
The optimal type of esophagectomy and extent of lymphadenectomy for patients after neoadjuvant chemoradiotherapy (nCRT) for esophageal squamous cell carcinoma remain controversial. We hypothesized that a more radical resection is associated with better survival.
Methods
Data of patients who received nCRT followed by resection for esophageal squamous cell carcinoma between 2012 and 2021 were analyzed. Modified en bloc esophagectomy (mEBE) involves total mediastinal lymphadenectomy and resection of all periesophageal node-bearing tissues. Perioperative outcomes and survival rates of mEBE were compared with those of conventional esophagectomy (CE).
Results
A total of 238 patients were included. Compared with CE, mEBE was associated with a longer operative time, higher total number of resected lymph nodes, fewer complications, and less anastomotic leakage; length of stay was similar between the 2 groups. There was no difference in overall survival rates between patients with ypT0 N0 stage in the mEBE and CE groups; however, in patients with non–ypT0 N0 stage in the mEBE and CE groups, the 3-year overall survival rates were 58.5% and 28.5%, respectively (P < .001). On disease-free survival analysis, no difference was observed in patients with ypT0 N0 stage, whereas patients with non–ypT0 N0 stage after nCRT had significantly better disease-free survival after mEBE compared with CE (49.7% vs 27.2%; P = .017).
Conclusions
Survival after mEBE was significantly better than that after CE. The mEBE did not increase postoperative hospital stay and complication rates.
新辅助放化疗后,全纵隔淋巴结切除术和食管周围淋巴结组织切除术的改良en-block切除 可提高术后生存,特别是非PCR患者。
原文链接:http://www.xxwk.net/archives/3568