The Belsey Mark IV repair or antireflux fundoplication is a classic procedure that has proven to be a successful and durable antireflux operation. Over a 15-year period, Ronald Belsey performed clinical trials to develop and refine the operation, culminating in 4 iterations, with the fourth or Mark IV being the final and most successful. Dr Belsey referred to each version as Mark as a nod to the British Jaguar brand automobile makers for naming their sequential iterations of luxury vehicles Mark I, Mark II, etc. The open Belsey Mark IV fundoplication (BMIV) is performed via a left posterolateral thoracotomy. The goal is to return the “high-pressure zone” of the cardia, otherwise known as the lower gastroesophageal sphincter (LES) to its normal anatomical position below the diaphragm. The BMIV reduces 4-5 cm of distal esophagus to an infradiaphragmatic position in the “high-pressure” upper abdomen, restoring a competent gastroesophageal junction (GEJ). In addition to returning the LES to a high-pressure environment, the BMIV provides an incomplete 240° anterior fundal wrap. The incomplete wrap, as opposed to a complete 360° Nissen fundoplication, is especially useful in the esophagus with underlying motility disorder, avoiding gas bloat syndrome.
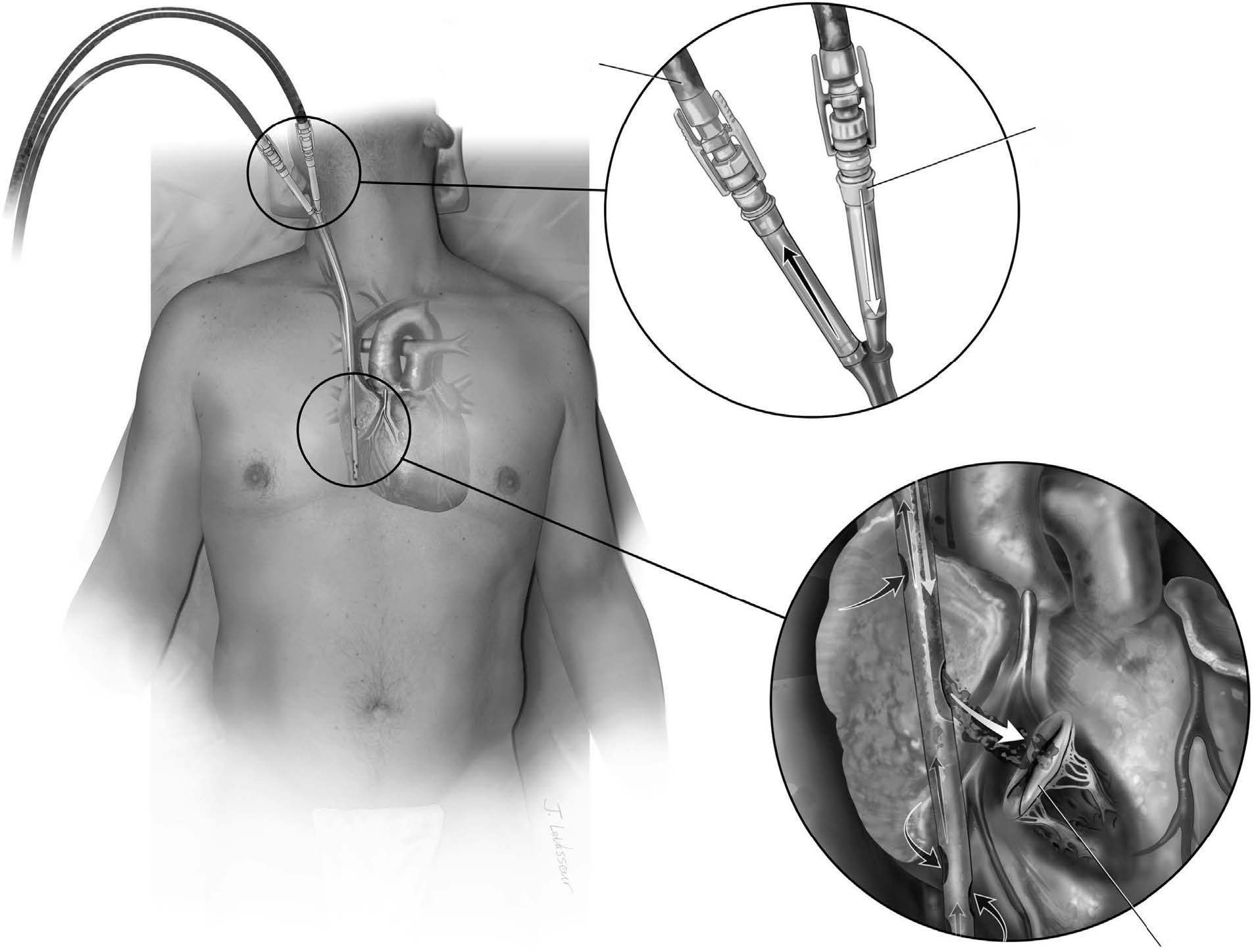
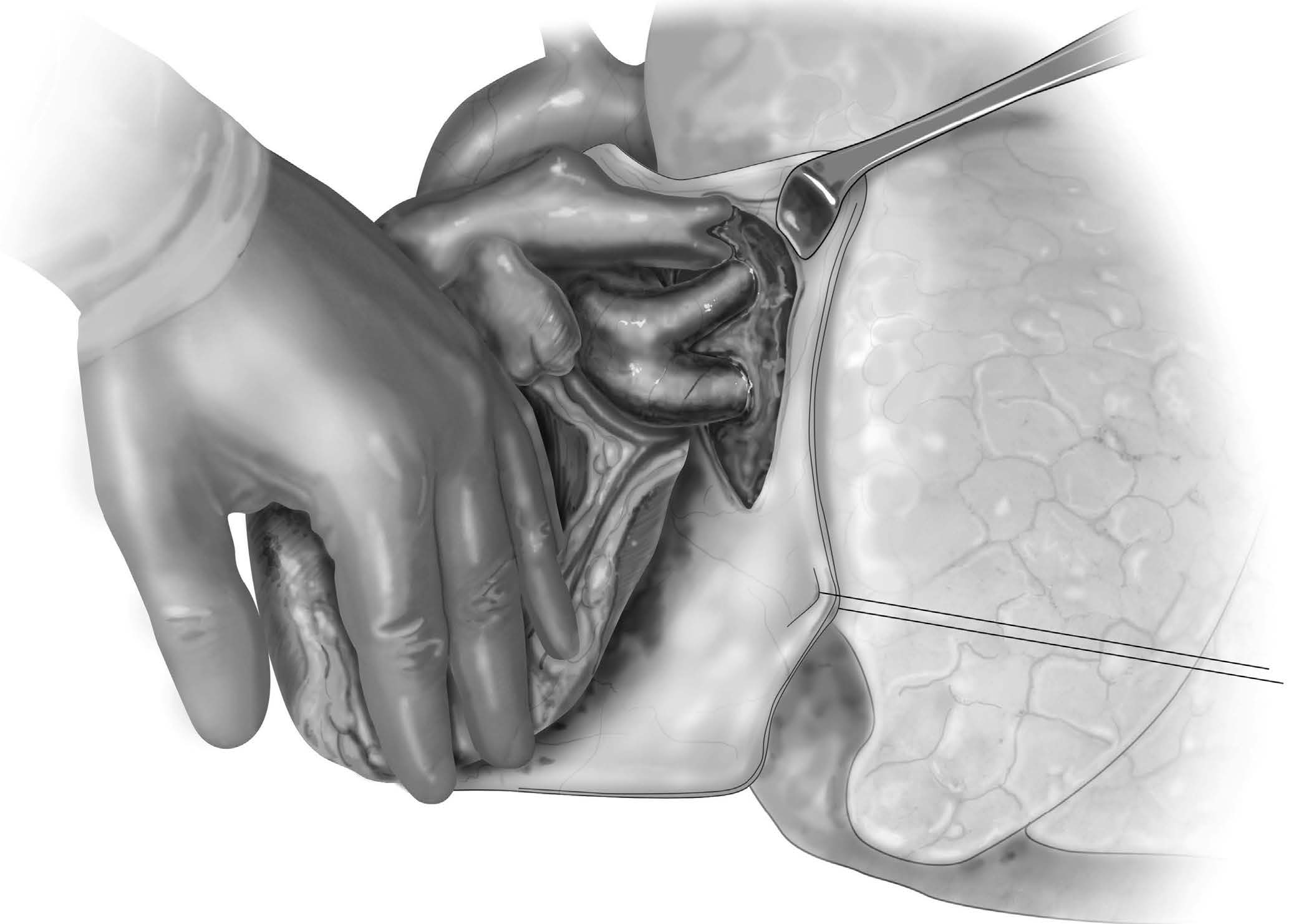
Orringer et al1 reported Belsey’s short- and long-term results in 892 patients, with 84% perceiving excellent or good results, and found a 12% 10-year recurrence rate and 14.7% recurrence rate for patients followed up over 10 years. Operative mortality was only 1%. Similar results in other studies have been reported with low operative mortality and success rates up to 90%.2With the proliferation of minimally invasive surgery, specifically conventional and robotic laparoscopic surgery, the role of the BMIV has diminished. Incomplete fundoplications such as the 180°-200° Dor anterior and the 270° Toupet posterior fundoplications are easily accomplished minimally invasively. Nguyen et al3 reported on their group’s initial experience with a thoracoscopic BMIV, and although their study demonstrated that a thoracoscopic BMIV could be performed with optimal perioperative mortality and morbidity, the complexity of the procedure warranted the authors to state an “open thoracotomy for Belsey Mark IV should remain the standard operation for gastroesophageal reflux disease with poor esophageal motility when a thoracic approach is desired.” Regarding BMIV, it is best approached via an open left posterolateral thoracotomy, and appropriate patients should be selected who would benefit from an antireflux procedure using a partial wrap and a thoracotomy.2, 4 Such patients include those with epiphrenic diverticulum,5 giant hiatal hernia with potential pleural adhesions and not requiring a gastric lengthening procedure, and esophageal perforation in the setting of esophageal dysmotility such as achalasia or diffuse esophageal spasm.6, 7 For patients who require an esophageal lengthening procedure, a Collis gastroplasty should be favored over a BMIV.2Preoperative assessment is determined by the underlying pathology. Flexible endoscopy, contrast esophagography with thin barium, and chest computed tomography are all employed for anatomical definition and surgical planning. Esophageal manometry identifies underlying esophageal dysmotility. In the following sections, we describe the open BMIV, which consists of 3 major steps: (1) narrowing a potentially patulous esophageal hiatus, (2) creating a 240° anterior fundoplication, and (3) securing the fundoplication in an infradiaphragmatic position therefore recreating the high-pressure zone of the LES.
原文链接:http://www.xxwk.net/archives/1737